
Endovascular Aneurysm Repair (EVAR)
Endovascular Aneurysm Repair (EVAR) is a minimally invasive procedure designed to treat aortic aneurysms—especially those occurring below the kidneys, known as Abdominal Aortic Aneurysms (AAA).
An aortic aneurysm develops when the artery wall weakens, causing a balloon-like bulge that can enlarge over time. If left unaddressed, a large aneurysm may rupture, leading to internal bleeding and life-threatening complications. By reinforcing the weakened section of the aorta with a stent-graft, EVAR aims to prevent further expansion and significantly reduce the risk of rupture.
Why Choose EVAR?
Over the past few decades, EVAR has become a popular alternative to open surgery for abdominal aortic aneurysms, largely due to its minimally invasive nature. Small incisions—usually in the groin—allow the surgeon to place a stent-graft inside the weakened artery without the extensive incisions required for traditional repair.

In the EVAR procedure, a covered stent graft is inserted into the aorta through small incisions in the groin.
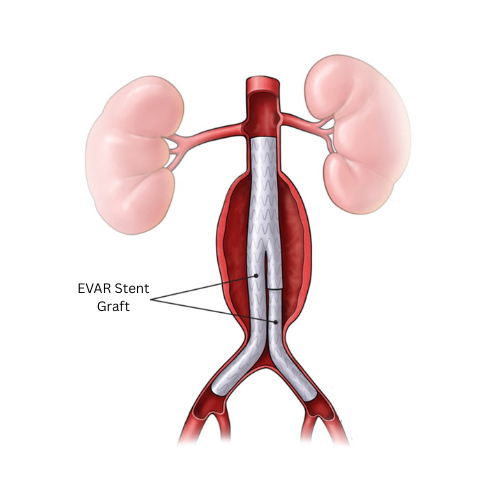
The EVAR covered stents reinforce the weakened wall and redirects blood flow through new channels, reducing pressure on the aneurysm.
Patients often find that EVAR offers several advantages:
- Shorter Recovery and Hospital Stay: In many cases, hospitalization lasts just a few days, and most individuals return to their usual activities much sooner than they would after open surgical repair.
- Lower Early Surgical Risk: EVAR can be a safer choice for patients with additional health concerns, such as heart or lung conditions that make lengthy surgery riskier.
- Reduced Pain and Discomfort: Because the procedure uses small incisions rather than a large abdominal incision, patients often experience less post-operative pain.
Although EVAR boasts a strong safety profile, it is not universally appropriate. Certain anatomical factors—such as the shape, size, or location of the aneurysm—may limit the feasibility of placing the stent-graft securely. In some cases, conventional open repair yields a longer-lasting fix. A comprehensive evaluation by your vascular surgeon, taking into account your overall health and the characteristics of your aneurysm, will help determine the best course of action.
The Aortic Stent-Graft: How It Works
A central component of EVAR is the stent-graft, a tube-like structure composed of a metal framework (the “stent”) covered by a fabric graft. This stent-graft is introduced through the femoral arteries in the groin and guided into the abdominal aorta under real-time X-ray imaging. Once placed inside the aorta, the stent-graft expands and fits snugly against the artery wall, creating a new pathway for blood flow. By diverting blood away from the weakened section of the aorta and relieving pressure on the bulging area, EVAR substantially lowers the likelihood of rupture.
To ensure a successful procedure, the stent-graft must be carefully sized to match the patient’s aorta. Pre-procedure planning often involves a CT scan that provides highly detailed images of the aneurysm’s dimensions, helping the vascular surgeon select a device with the right length and diameter. This meticulous fitting process is crucial for ensuring that the stent-graft remains stable over time and that the blood is effectively rerouted through the newly created channel.
Planning for EVAR
Before undergoing Endovascular Aneurysm Repair (EVAR), you will typically have one or more imaging tests—most often a CT scan—to map out the size, shape, and location of your aneurysm. This detailed information allows your vascular surgeon to select a stent-graft that precisely fits your aorta, ensuring it stays in place and effectively reroutes blood away from the weakened area.
During this preparatory phase, you may also undergo blood tests and other evaluations to confirm you’re in good condition for surgery. Proper sizing and thorough assessments are key to a successful procedure and help minimize any risks once the stent-graft is placed.
The EVAR Procedure
EVAR is typically performed under general anesthesia, although some high-risk patients may be candidates for spinal anesthesia or sedation. Once you are anesthetized, your surgeon makes small incisions in the groin area to access the femoral arteries. Under the guidance of real-time X-ray imaging, a flexible catheter is advanced through these arteries until it reaches the aneurysm within the aorta.
A stent-graft is then placed inside the aneurysm. When properly positioned and released, the stent-graft expands against the artery walls, essentially bypassing the weakened section of the aorta and reducing pressure on the aneurysm. Once the surgeon is satisfied with the stent-graft’s placement, the catheter is withdrawn and the small incisions in your groin are closed.
Recovery and Follow-Up
After EVAR, most patients stay in the hospital for two to three days, though some might require a longer stay if they have underlying health issues. Post-operative monitoring may include a stint in a high-dependency ward or even the ICU for individuals at higher risk. Once discharged, you will receive instructions on caring for your incisions, gradually resuming physical activities, and scheduling follow-up imaging to verify that the stent-graft remains well-positioned.
Over time, periodic scans are essential to detect any issues such as endoleaks, which may occur when blood leaks around or within the stent-graft. Though EVAR typically carries a lower early surgical risk than open repair, it does require lifelong follow-up. Complications, while infrequent, can include infections, stent-graft movement, and endoleaks. Carefully adhering to your doctor’s advice and attending all recommended check-ups play a key role in minimizing these risks.
If you’d like to explore whether Endovascular Aneurysm Repair is the right option for your aortic aneurysm, reach out to Dr. Darryl Lim to schedule a consultation and discuss a personalized treatment plan that aligns with your medical needs and lifestyle.
This information is provided as a general guideline and should not replace professional medical advice. Always consult your healthcare provider for personalized recommendations.
FAQ's about Endovascular Aneurysm Repair (EVAR)
EVAR is a minimally invasive procedure used to treat aortic aneurysms, specifically those in the abdominal and chest region, by reinforcing the weakened portion of the aorta with a stent-graft.
- EVAR involves smaller incisions and is generally less invasive than open surgery, which usually involves a large incision in the abdomen.
- Advantages of EVAR include a shorter recovery period, less pain post-operation, reduced risk of complications during and after the procedure, and its suitability for high-risk patients.
- An ideal candidate for EVAR is typically an individual with an abdominal aortic aneurysm, particularly those at higher risk for traditional open surgery due to factors such as age and underlying medical co-morbidities. Additionally, the candidate should have a favorable aortic anatomy that would permit a secure seal of the stented portion.
The EVAR procedure entails making a small incision in the groin through which a catheter is inserted. A stent-graft is then guided to the appropriate location to seal off the aneurysm and divert blood flow away from it, all under the meticulous guidance of real-time X-ray imaging.
Following the procedure, you will be monitored in the recovery room before being transferred to a standard hospital room. High-risk patients may require a stay in a High-Dependency ward or possibly the Intensive Care Unit (ICU) for closer post-operative monitoring.
You should be able to walk the day after the procedure and expect to be discharged within 2-3 days. Recovery after EVAR typically involves shorter hospital stays and less pain compared to open surgery. While there will be some initial restrictions on physical activity, most patients can return to their normal activities within a few weeks.
Even though EVAR is a minimally invasive procedure, it is still considered major surgery. As with all surgeries, inherent risks are involved. Some of the risks specific to EVAR include endoleak, infection, and complications related to the stent, such as fractures, blockages, or migration.
Dr. Lim will thoroughly discuss the potential risks and tailor an individualized treatment plan should you require this surgery.
Follow-up after EVAR typically involves regular imaging tests, such as CT scans, to ensure the stent-graft remains in place without leakage (referred to as ‘endoleak’) and to verify that the aneurysm is not expanding.
Embracing certain lifestyle alterations, such as adopting heart-healthy habits and incorporating regular exercise, might be advised after undergoing EVAR. Maintaining optimal blood pressure control also plays a pivotal role in ensuring favorable long-term outcomes post-procedure.
EVAR has proven to be highly effective in treating abdominal aortic aneurysms, preventing rupture, and providing a minimally invasive alternative to open surgery in specific cases.
Yes, however, the suitability of EVAR for complex aneurysms hinges upon specific anatomical and medical considerations, meticulously evaluated by your vascular surgeon.
Dr. Lim, having accrued extensive experience in strategizing and executing EVAR for patients with potentially complex or atypical aneurysms, welcomes the opportunity to discuss your situation should you require such a procedure.
Costs for EVAR can vary, influenced by factors such as the hospital and insurance coverage. While most insurance plans do cover EVAR, consulting with your insurance provider is essential.
An EVAR typically takes approximately 1-3 hours, with the duration varying based on the anatomical complexity of the aneurysm.
Open aortic repair surgery serves as the primary alternative to EVAR, especially for aneurysms with an anatomy unsuitable for stenting.
Yes, but anticipate some temporary restrictions following surgery. After an initial recovery period, most patients are able to resume their regular physical activities within 1-2 weeks.
Stent-grafts used in EVAR are typically composed of a metal framework, often made from stainless steel or nitinol, and are covered with synthetic fabric. The exact materials can vary depending on the manufacturer.
For instance, the Endurant stent-graft from Medtronic has components made of nitinol metal stents, which are sewn onto a multifilament polyester (PET [polyethylene terephthalate]) graft fabric.
The stent-graft used in EVAR reinforces the aorta by redirecting blood flow within the stent, which alleviates pressure on the aneurysm wall and consequently minimizes the potential for rupture.
EVAR has generally high success rates, with low early mortality and quick recovery periods.

