
Summary:
May-Thurner syndrome, also called iliac vein compression syndrome, occurs when the right common iliac artery compresses the left common iliac vein in the pelvis, reducing venous drainage from the left leg. This can cause blood to pool and pressure to build up, leading to left leg swelling, heaviness, aching, venous claudication, varicose veins, or left-sided deep vein thrombosis. Seek assessment if one leg is persistently more swollen or painful than the other, or if you have an unexplained or recurrent DVT. Diagnosis is with duplex ultrasound and, when needed, CT/MR venography, venography, and IVUS. Treatment strategies may include minimally invasive iliac vein angioplasty and stenting.
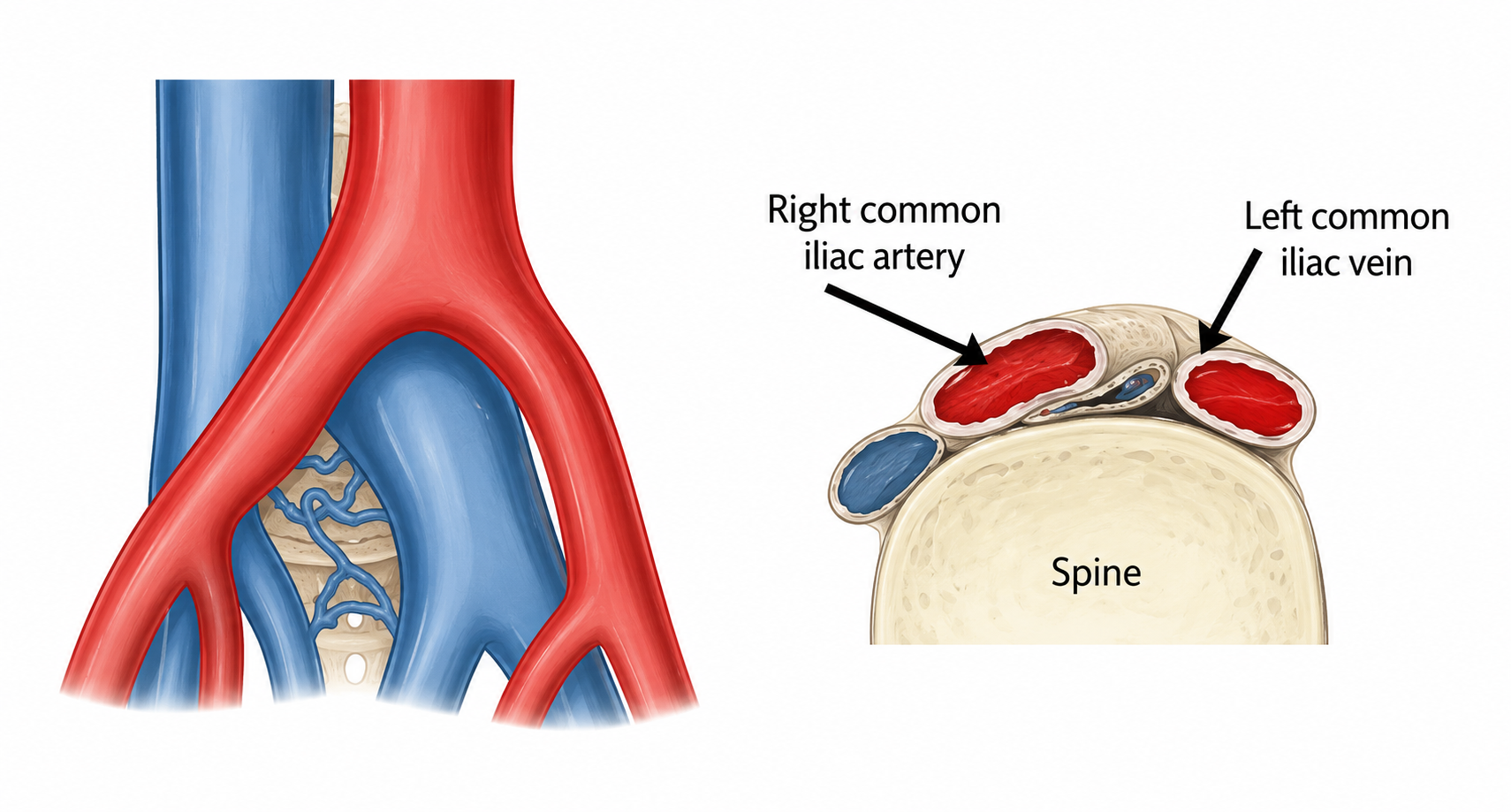
May-Thurner syndrome, also called iliac vein compression syndrome, happens when the right common iliac artery compresses the left common iliac vein in the pelvis. This can slow blood flow from the left leg and pelvis, leading to venous hypertension, leg swelling, pain, heaviness, varicose veins, or even deep vein thrombosis (DVT). Importantly, some people have this vein compression anatomy without symptoms, so the diagnosis of May-Thurner syndrome should be based on both symptoms and imaging, not on an incidental scan finding alone.
May-Thurner syndrome is under-recognised because its symptoms can overlap with more common conditions such as simple leg swelling, chronic venous insufficiency, or DVT. In women, it can also overlap with pelvic venous disorders and sometimes contribute to chronic pelvic pain or pelvic congestion syndrome. At Dr Darryl Lim’s clinic in Singapore, our goal is to identify whether iliac vein compression is truly the cause of your symptoms and, if so, plan treatment that is targeted, evidence-based, and as minimally invasive as possible.
Causes and Risk Factors
May-Thurner syndrome develops because the left common iliac vein lies beneath the right common iliac artery and in front of the lower lumbar spine. Repeated arterial pulsation can cause chronic mechanical pressure and injury to the vein wall over time, contributing to scar-like thickening or intraluminal “spurs”. These changes can narrow the vein enough to impair venous outflow from the left leg and sometimes the pelvis.
Not everyone with this anatomy develops symptoms. Many people have iliac vein compression without ever knowing it- in one CT study of asymptomatic patients, 24% had greater than 50% compression of the left common iliac vein. Symptoms usually become clinically apparent when the compression is significant enough to impair blood flow or when another “stressor” or risk factor tips the balance toward clot formation.
Common situations that can unmask or worsen symptomatic May-Thurner syndrome include prolonged immobility, long travel, dehydration, recent surgery, a pro-thrombotic tendency (ie easy blood “clotting”), pregnancy, and the postpartum period. The syndrome is often recognised in younger to middle-aged women, but it can also occur in men. The condition should especially be considered when there is unexplained or recurrent left leg DVT.
Symptoms and Warning Signs
The most common symptoms occur on the left leg. Patients may notice one leg swelling more than the other, a feeling of heaviness, aching, tightness, or a dragging discomfort that worsens after prolonged standing or walking (especially at the end of the day). Some patients also develop venous claudication, which means leg pain or bursting discomfort during activity because venous outflow is restricted. In chronic cases, there may be visible varicose veins, skin discolouration, or even venous ulceration.
A major concern is deep vein thrombosis. If a clot forms in the compressed vein system, symptoms can become much more dramatic, with sudden swelling, pain, warmth, and tenderness in the affected leg. DVT matters not only because it causes acute symptoms, but also because it can increase the risk of pulmonary embolism and long-term post-thrombotic syndrome if not recognised and treated properly.
Pelvic symptoms can also occur, although they are less typical than leg symptoms. In some women, May-Thurner syndrome can contribute to pelvic venous hypertension and overlap with pelvic congestion syndrome. In these patients, symptoms may include chronic pelvic heaviness, pelvic pain worse with prolonged standing, dyspareunia (pain during intercourse), vulval or upper-thigh varicose veins.
There are some red flag symptoms to take note of. You should seek urgent medical attention if you have sudden one-sided leg swelling, severe leg pain, a painful blue or pale swollen leg, chest discomfort or breathlessness. These features may indicate acute DVT or pulmonary embolism and should not be monitored at home.

How May-Thurner Syndrome Is Diagnosed
Diagnosis starts with history and examination, but imaging is essential. A venous duplex ultrasound is usually the first imaging test because it is non-invasive and useful for detecting DVT, venous reflux, and signs that suggest proximal outflow obstruction. However, ultrasound can be limited for May-Thurner syndrome because the compressed iliac vein lies deep in the pelvis and may not be directly visualised well.
When there is a high suspicion of iliac vein compression, a CT Venogram or MR Venogram is usually the next step. Cross-sectional imaging can show the site of compression, collaterals, associated DVT, and alternative causes such as masses or lymphadenopathy.
A diagnostic venogram and intravascular ultrasound (IVUS) are most useful when intervention is being planned or when uncertainty remains after noninvasive imaging. Venography provides dynamic luminal imaging and can be combined with treatment in the same session, but it often underestimates disease severity compared with IVUS. IVUS is the most sensitive intraprocedural test for iliac vein compression, and is especially useful for confirming the stenotic lesion, sizing the vein, and choosing accurate stent landing zones.
A useful way to think about the diagnostic pathway is this: ultrasound is usually the starting point, CT or MR venography helps define the pelvic vein compression more clearly, and venography with intravascular ultrasound (IVUS) is often the final confirmatory step when stenting or other treatment is being considered.
Treatment Options for May-Thurner Syndrome
Treatment for May-Thurner Syndrome depends on your symptoms. The most suitable treatment option depends on whether you have an incidental compression finding, symptomatic non-thrombotic obstruction, acute deep venous thrombosis (DVT), chronic post-thrombotic symptoms, or associated pelvic venous disease. Current guidelines are clear that asymptomatic patients should not be offered venous stenting, while symptomatic patients with clinically symptomatic outflow obstruction may benefit from endovascular treatment.
Asymptomatic – Conservative management
If symptoms are mild, or if compression is found incidentally without convincing clinical features, conservative management may be appropriate. This can include compression stockings, keeping mobile, leg elevation when practical, hydration, and reducing prolonged immobility such as during long travel. These measures do not remove the underlying compression, but they may reduce venous pooling and improve symptoms in selected patients.
Symptomatic, Non-Thrombotic – Iliac Vein Angioplasty and Stenting
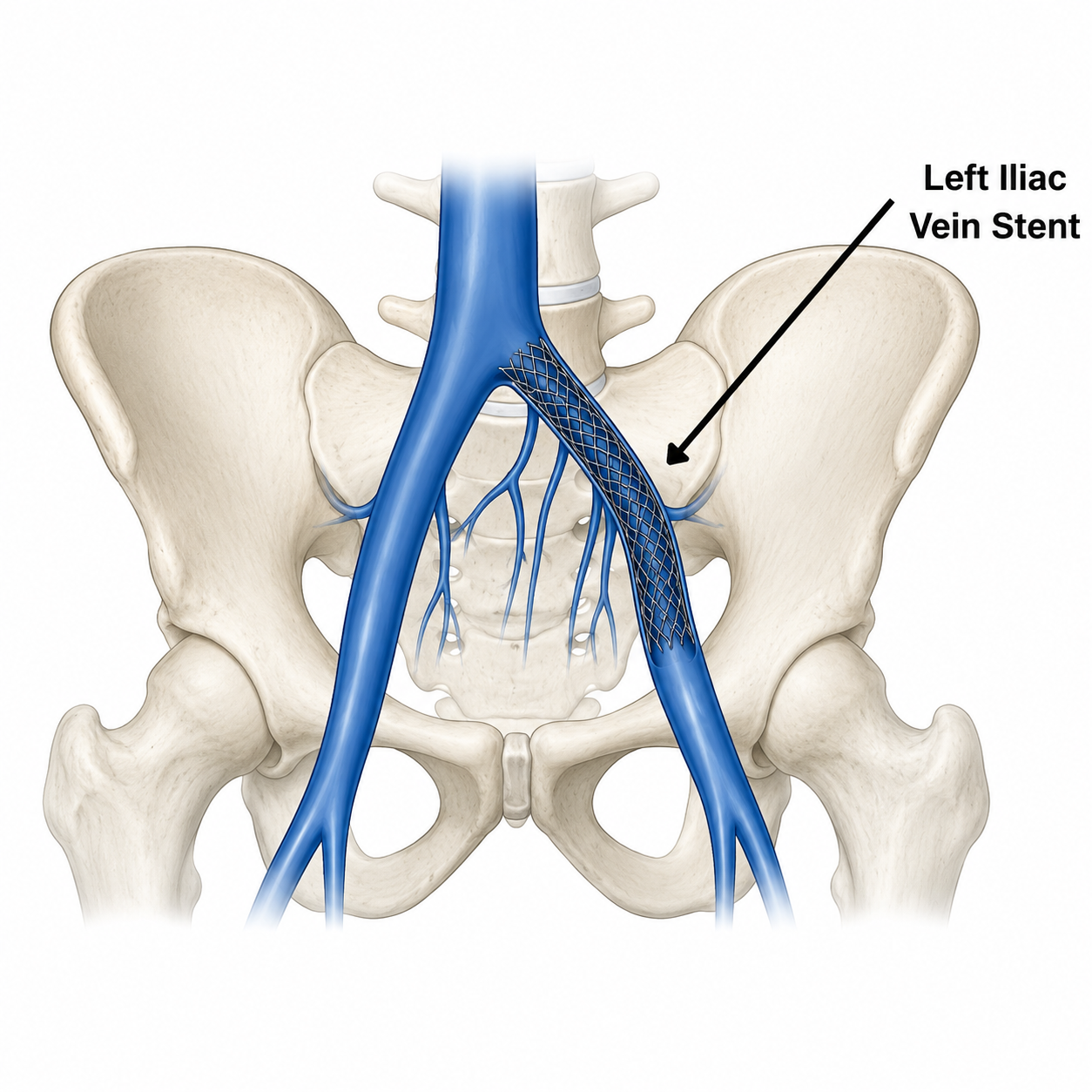
For symptomatic non-thrombotic May-Thurner syndrome, the main definitive endovascular treatment is iliac vein stenting. This is a minimally invasive “keyhole” procedure performed through a small puncture in each groin. Venography and IVUS are used to map the culprit lesion, a balloon is used to open the narrowed segment, and a venous stent is placed to keep the vein expanded against the ongoing external compression.
Thrombotic (when acute DVT is present)
(i) Anticoagulation
If the presentation is that of a DVT in the leg, blood thinners are usually needed to prevent clot extension and reduce the risk of pulmonary embolism. It is important to understand that anticoagulation treats the clotting risk, but it does not correct the mechanical compression itself. That is why some patients with acute iliofemoral DVT may also need catheter-based clot removal and treatment of the underlying iliac vein obstruction.
(ii) Minimally invasive catheter-directed thrombolysis or thrombectomy
In selected patients with acute iliofemoral DVT, especially when symptoms are severe and the clot burden is extensive, catheter-based thrombolysis or thrombectomy may be considered. If a significant culprit iliac vein lesion is identified during treatment, current guidelines support considering venous stenting rather than leaving the obstruction untreated. This is particularly relevant for reducing ongoing outflow obstruction and long-term post-thrombotic morbidity.
Treatment of associated Pelvic Congestion Syndrome
If imaging shows that iliac vein compression is contributing to pelvic venous hypertension, varices, or pelvic congestion symptoms, further treatment may be needed beyond the iliac stent. Depending on the venous pattern, this may involve staged management of associated pelvic reflux or embolisation of faulty pelvic veins. The exact sequence is individualised and should follow a full venous work-up rather than a one-size-fits-all pathway.
Open or Hybrid Surgery
Open surgical reconstruction is now uncommon and generally reserved for a very small group of patients in whom endovascular options are unsuitable, have failed, or do not fully address the anatomy. Current European guidance places surgery behind endovascular treatment for most significant iliac outflow obstruction.
Recovery and Long-Term Outlook
One of the advantages of modern venous intervention is that it is usually much less invasive than open surgery. Most patients recover much faster after minimally-invasive treatment, although the exact recovery depends on whether the treatment involves simple stenting, or more extensive thrombectomy for acute DVT. Mild post-procedure back, groin, or pelvic discomfort can occur, and close follow-up is important to confirm symptom improvement and stent patency.
Long-term outcomes are generally strongest when the right patients are selected for treatment. Guidance and reviews consistently recommend follow-up after stenting, multidisciplinary management, and an individualised antithrombotic plan. The exact post-stent blood thinner or antiplatelet regimen is not universal and should be tailored to whether the patient had DVT, the type of lesion, bleeding risk, and other medical factors.
Compassionate, Specialist Care in Singapore
If you have persistent left-leg swelling, heaviness, non-healing ulcers or a history of recurrent left-sided DVT, May-Thurner syndrome is worth assessing properly. At Dr Darryl Lim’s clinic, the aim is not simply to find compression on a scan, but to determine whether it is truly driving your symptoms and whether conservative care, surveillance, or minimally invasive treatment is the right next step. When needed, care can be coordinated with other specialists (such as hematology) to ensure that treatment is both safe and appropriately targeted.
FAQ about May-Thurner Syndrome
What is May-Thurner syndrome?
It is a condition in which the right common iliac artery compresses the left common iliac vein, reducing venous outflow from the left leg and sometimes the pelvis. It is also called iliac vein compression syndrome.
What symptoms can it cause?
Common symptoms include left-leg swelling, heaviness, aching, exercise-related discomfort, varicose veins, skin changes, ulceration or DVT. In some patients, it can also contribute to pelvic venous symptoms.
Can May-Thurner syndrome cause DVT?
Yes. The compression can slow venous flow and increase the risk of left-sided iliofemoral DVT, particularly when other clotting risks are present.
How is it diagnosed?
Diagnosis often starts with duplex ultrasound. CT or MR venography may then be used to map the anatomy, and venography with IVUS is often used when intervention is being planned.
Does everyone with iliac vein compression need a stent?
No. Current guidance recommends against intervention for asymptomatic lesions. Stenting is generally reserved for patients with clinically significant symptoms or obstruction.
Can May-Thurner syndrome cause pelvic pain?
It can in some patients, particularly when iliac vein obstruction contributes to pelvic venous hypertension or pelvic congestion. Other pelvic causes should still be ruled out first.
Will I need blood thinners after treatment?
That depends on your case. Patients with DVT often need anticoagulation, but the exact medication and duration after venous stenting are individualised.
When should I seek urgent care?
Seek urgent medical review if you develop sudden one-sided leg swelling, severe leg pain, chest pain, breathlessness, or coughing up blood.










