Not every varicose vein needs treatment straight away.
Some people have mild varicose veins for years with little discomfort, no swelling and no skin changes. In that situation, monitoring and conservative measures may be perfectly reasonable.
However, varicose veins should not automatically be dismissed as “just cosmetic”. In many patients, they are a sign of venous reflux, where the valves in the leg veins do not close properly and allow blood to pool in the legs. Over time, this can lead to aching, swelling, skin damage, inflammation, bleeding or venous ulcers.
The real question is not simply: “Do I have varicose veins?”
But should be: “Are these veins causing symptoms, or showing signs of progression that may put me at risk of complications?”
In this article, Dr Darryl Lim, a vascular and varicose vein specialist in Singapore, explains when varicose veins can be monitored, when treatment is worth considering and how duplex ultrasound helps guide the decision.

What are varicose veins?
Varicose veins are enlarged, twisted veins that appear under the skin, most commonly on the legs. They develop when the one-way valves inside the veins weaken. Normally, these valves help keep blood flowing upwards towards the heart. When they fail, blood falls backwards and pools in the leg. This is known as venous reflux.
Over time, the affected veins stretch and become more visible. Some people mainly notice their appearance, while others develop heaviness, aching, swelling, itching, night cramps or skin changes around the ankles.

The visible varicose veins are often only the surface sign. The underlying reflux may be coming from underlying larger superficial veins (such as the great saphenous vein, small saphenous vein or accessory veins).
When can varicose veins be left alone?
Monitoring without active treatment may be reasonable when the veins are small, stable and not causing meaningful symptoms. There should also be no persistent swelling, skin changes, bleeding or previous episodes of thrombophlebitis.
In these situations, regular walking, leg elevation, weight management and compression stockings may help keep symptoms controlled.
Pregnancy is another common situation where definitive treatment is often postponed. Pregnancy-related varicose veins may improve after delivery (once hormone levels revert to pre-pregnancy levels), so it is usually sensible to allow time for natural recovery unless complications develop.
Some patients may also choose not to undergo treatment after understanding the benefits and risks. That is reasonable, provided they know what changes should prompt reassessment.
When is treatment worth considering?
Treatment becomes more relevant when the veins are causing symptoms, affecting daily life or showing evidence of progression.
Persistent symptoms
Common symptoms include:
– Aching, heaviness or throbbing
– Ankle or lower-leg swelling
– Night cramps or restless legs
– Itching or burning along a vein
– Sensation of tightness or pressure

These symptoms often worsen after prolonged standing or sitting and improve with walking or leg elevation. If they are interfering with work, sleep, exercise or daily comfort- it is worth assessing whether underlying reflux should be treated.
Skin changes
Changes around the ankle or lower leg are an important warning sign. These may include brown pigmentation, venous eczema, persistent itching, dry skin, hardening of the tissues or lipodermatosclerosis.
Once the skin is affected, the condition has progressed beyond uncomplicated visible veins. Treatment may help reduce venous pressure and prevent further deterioration.

Venous ulcers
A venous ulcer is a slow-healing wound, usually near the ankle, caused by long-standing venous pressure.
Active or previously healed venous ulcers are a clear reason to assess the underlying reflux. Treating the reflux does not replace wound care, but it may improve healing conditions and reduce the risk of the ulcer returning.
Superficial thrombophlebitis
Superficial thrombophlebitis is inflammation and clotting within a surface vein. It often feels like a painful, red, warm and hardened cord along a varicose vein.
A single mild episode may settle with treatment, but recurrent episodes suggest that the underlying varicose veins should be assessed.
Bleeding
A varicose vein close to the skin can bleed after relatively minor trauma, particularly around the ankle where the skin may already be thin or damaged.
If this happens, lie down, elevate the leg and apply firm direct pressure. Even if the bleeding stops, vascular assessment is important because it may recur.
Recurrent varicose veins
Varicose veins can return years after previous treatment because of new reflux, residual reflux or more commonly- the development of new vein pathways.
A repeat duplex ultrasound is usually needed before deciding whether further treatment is worthwhile.
Will untreated varicose veins always get worse?
Not always.
Some mild varicose veins remain stable for years. Others gradually become more prominent and symptomatic, with increasing heaviness, swelling or skin changes. A smaller group may progress more quickly following pregnancy, weight gain, prolonged standing work or an episode of thrombophlebitis.

Factors that may increase the likelihood of progression include:
- Significant reflux on duplex ultrasound
- Symptoms that are worsening over time
- Existing skin changes or swelling
- Obesity
- Prolonged standing or sitting
- Older age
- Previous venous ulceration
- Strong family history of advanced venous disease
Possible complications include venous eczema, brown ankle pigmentation, lipodermatosclerosis, superficial thrombophlebitis, bleeding and venous ulceration.
This does not mean that every untreated varicose vein will cause a complication. The purpose of assessment is to distinguish mild disease that can be observed from reflux that is already causing damage.
Why having a Duplex Ultrasound Scan matters
A proper varicose vein assessment involves more than looking at the visible veins.
A duplex ultrasound checks whether the valves are functioning properly and maps where reflux is coming from. It helps answer several important questions:
- Is significant venous reflux present?
- Which are the problematic veins?
- Are the visible veins connected to a larger refluxing vein?
- Is the problem medically significant or mainly cosmetic?
- What treatment plan would best match the particular patient’s anatomy of diseased veins?
Dr Darryl Lim will usually recommend duplex ultrasound when there are significant varicose veins, persistent symptoms, swelling, skin changes or complications. The scan allows treatment to target the true “root” source of the problem rather than simply removing visible veins.
What can conservative measures achieve?
Conservative measures can be useful, particularly for mild symptoms or for patients who prefer to avoid procedures.
Regular walking and calf exercises support the natural calf-muscle pump, which helps pump blood out of the lower legs. Elevating the legs can reduce swelling, while weight management may lower pressure within the veins. Avoiding long periods of sitting or standing without movement can also reduce pooling.
Compression stockings provide external support and may improve aching, heaviness and swelling while they are worn.
However, these measures do not repair faulty valves or make established varicose veins disappear. When the stockings are removed, the underlying reflux remains.
Conservative care is therefore best viewed as a way to manage symptoms rather than permanently correct the cause.

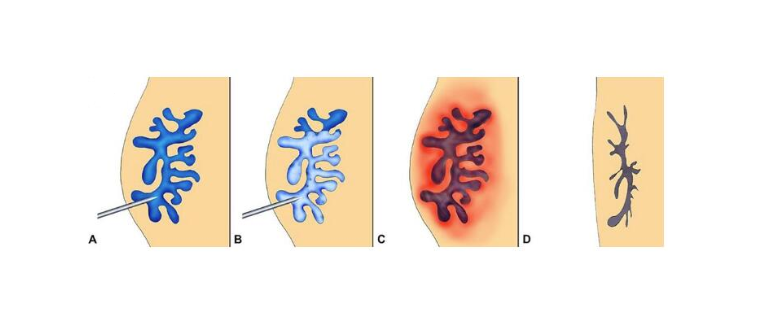
What treatments are available?
Modern varicose vein treatment is usually minimally invasive and commonly performed as day surgery. The aim is to close or remove the diseased refluxing veins so blood reroutes through healthier veins.
Treatment options include:
– Radiofrequency Ablation (RFA), which utilizes heat to seal the refluxing vein from inside.
– VenaSeal, which uses a medical adhesive “glue” to close the vein without heat.
– ClariVein mechanochemical ablation, which combines mechanical treatment with a sclerosant medication.
– Ultrasound-guided foam Sclerotherapy, which may be used for selected vein patterns, branches or residual veins.
– Mini Phlebectomies, where prominent surface veins are removed through tiny punctures.
– Traditional ligation and stripping is less commonly required today but may still be appropriate in selected cases.
The most suitable treatment depends on the ultrasound findings, vein size and location, symptoms, skin condition, patient preference and cost considerations.
Is cosmetic treatment a valid reason?
Yes. Cosmetic concern is a valid personal reason to seek treatment, particularly in Singapore where the legs are often visible in shorts, skirts and activewear.
However, it is important to distinguish cosmetic-only treatment from treatment for a medical condition.
If there are no symptoms, skin changes or significant reflux, treatment may be considered purely cosmetic. It is generally not MediSave-claimable and is usually not covered by insurance.
Some patients who initially seek treatment for appearance discover that they also have aching, swelling or ultrasound-confirmed reflux. In those cases, there may be both medical and cosmetic reasons for treatment.
A consultation and duplex ultrasound can clarify which part of the treatment is medically indicated.
What are the risks of treatment?
Modern varicose vein treatments are generally well tolerated, but no procedure is completely 100% risk-free.
Possible side effects include bruising, tenderness, tightness, superficial thrombophlebitis, pigmentation along the treated vein and recurrence over time.
Less common risks include allergic reactions to certain treatment agents, failure of the vein to close, nerve injury causing numbness or tingling, and deep vein thrombosis.
The exact risks vary according to the procedure and the patient’s anatomy. Treatment should therefore follow a proper discussion of the benefits, risks, alternatives and expected recovery.
How do you decide whether to treat?
The decision usually comes down to a few practical questions:
- Are the veins causing symptoms?
- Are the symptoms affecting daily life?
- Are there skin changes or complications?
- Does duplex ultrasound show significant reflux?
- Are conservative measures controlling the problem?
- Is the concern medical, cosmetic or both?
- What are the patient’s preferences and cost considerations?
There is rarely a need to decide immediately. Most patients can review the ultrasound findings, consider the options and make a decision after understanding what treatment can realistically achieve.
Patients who are unsure whether treatment is necessary can arrange a varicose vein consultation with Dr Darryl Lim for clinical assessment and duplex ultrasound where appropriate.
When should you see a vascular surgeon?
It is worth arranging an assessment if you have visible veins together with aching, heaviness, swelling, night cramps or itching. Skin pigmentation, eczema, hardening around the ankle, previous ulceration, recurrent thrombophlebitis or bleeding are stronger reasons not to delay.
Assessment is also useful when varicose veins have returned after previous treatment, or when cosmetic concerns are present and you want to know whether there is underlying reflux.
Early assessment does not automatically mean that you need a procedure. Sometimes the most appropriate plan is observation and conservative care. The aim is to understand the severity of the problem and identify any signs that treatment would be beneficial.
The bottom line
Varicose veins do not always need treatment.
Mild, stable veins without symptoms or skin changes can often be monitored. Walking, leg elevation, weight management and compression stockings may help control discomfort.
Treatment should be considered when varicose veins cause persistent pain, heaviness, swelling, night cramps, skin damage, thrombophlebitis, bleeding or venous ulcers. These signs suggest that the problem is no longer simply cosmetic.
A clinical assessment and duplex ultrasound provide the clearest way to determine whether the veins can be safely observed or whether treating the underlying reflux is worthwhile.
Frequently asked questions
Do varicose veins go away on their own?
Established varicose veins usually do not disappear on their own. Symptoms may improve with conservative measures, but the underlying structural valve damage remains.
Can varicose veins be left untreated?
Yes, if they are mild, stable, and not causing symptoms, swelling, skin changes, or complications. They should be reassessed if symptoms worsen.
Will untreated varicose veins always lead to ulcers?
No. Many patients never develop ulcers. However, the risk increases when significant reflux, chronic swelling, pigmentation, eczema, or skin hardening is present.
Can compression stockings replace treatment?
Compression stockings can reduce symptoms and swelling, but they do not repair faulty valves or remove varicose veins. They are useful for symptom control, but not a cure.
When should varicose veins be treated?
Treatment is usually considered when there is persistent pain, heaviness, swelling, night cramps, skin changes, thrombophlebitis, bleeding, ulcers, or significant reflux on ultrasound.
Is cosmetic treatment reasonable?
Yes. Cosmetic concern is a valid personal reason. However, purely cosmetic treatment is usually not MediSave claimable or insurance-covered unless there is a medical indication or relevant venous reflux symptoms.
Do varicose veins increase DVT risk?
Varicose veins may be associated with a modestly increased risk of DVT, especially with other risk factors such as immobility, surgery, hospitalisation, or previous clots. Individual risk should be assessed separately.
How often should varicose veins be reviewed if not treated?
For stable mild varicose veins, periodic review is reasonable. Earlier reassessment is needed if symptoms worsen, skin changes appear, or complications occur.